
technology
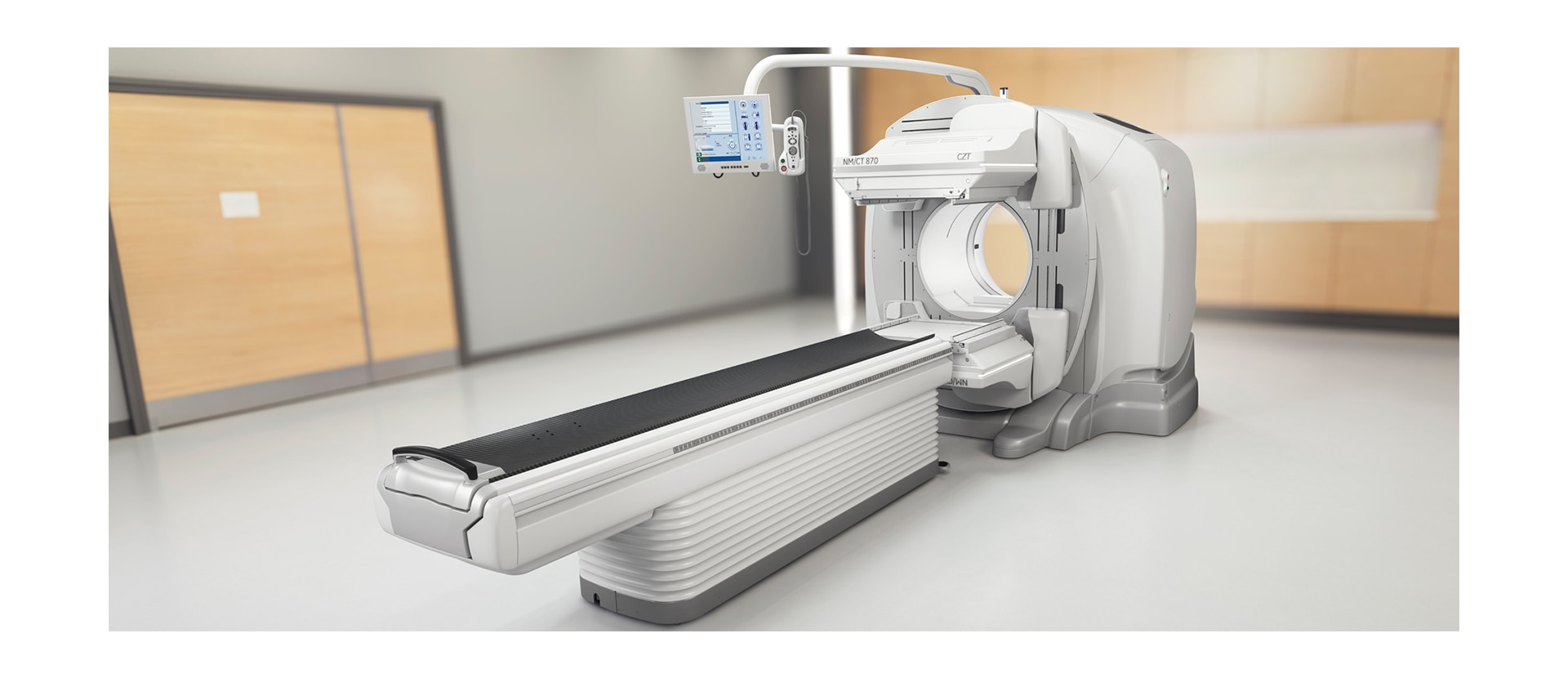
SPECT/CT as you have never seen it before

resolution
The resolution to discover something new
- Discover new protocols enabling differential diagnosis by visualizing multiple tracers simultaneously
- Push nuclear medicine’s boundaries by developing new diagnostic services
- Pursue opportunities for tracer development and better utilization of currently available tracers
- Continue your efforts to diagnose and stage disease earlier with smaller lesion detectability1
See everything clearly now
- More accurately assess treatment response to guide your treatment planning decisions with increased quantitation accuracy8
- Grow patient volumes from referring physicians that value accurate, reproducible results and the diagnostic confidence you deliver
- Increase patient satisfaction by reducing compromised exams that result in repeat scans

design
Designed to make every inch count
- Improve imaging results by scanning in closer proximity to your patients
- Provide more tolerable exams for greater patient comfort
$name
$name

quantitation
Quantitative SPECT/CT for every patient, every day
- Guide therapy planning decisions with quantitative disease state and treatment response assessments
- Grow patient volumes with referring physicians that value accurate, reproducible results and the diagnostic confidence you deliver
Built for quantitation
quantitative applications
Inform your decisions with measurable results
Q. Volumetrix MI
Q. Volumetrix MI
Q. Brain
DaTQUANT™
Q. Lung
Q. Lung
Dosimetry Toolkit
summary
A SPECT/CT system for true discovery
Related Products
- 1 In clinical practice, the use of NM/CT 870 CZT may improve lesion detectability depending on the clinical task, patient size, anatomical location and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose or scan time to obtain diagnostic image quality for the particular clinical task.
- 2 Together with Clarity 2D and Evolution5 and compared to Discovery NM/CT 670 Pro/ES/DR without Clarity 2D and Evolution5. As demonstrated in phantom testing using a bone scan protocol, and the NEMA IEC Body Phantom. The actual time/dose reduction depends on the clinical task, patient size, anatomical location and clinical practice.
- 3 At detector surface.
- 4 Demonstrated in phantom testing using NEMA IEC Body Phantom at 50% scan times with Evolution5. Compared to Discovery NM/CT 670 Pro/ES/DR.
- 5 In clinical practice, Evolution options5a (Evolution for Bone, Evolution for Cardiac, Evolution for Bone Planar) and Evolution Toolkit5b are recommended for use following consultation of a Nuclear Medicine physician, physicist and/or application specialist to determine the appropriate dose or scan time reduction to obtain diagnostic image quality for a particular clinical task, depending on the protocol adopted by the clinical site.
- 5a Evolution Options - Evolution claims are supported by simulation of count statistics using default factory protocols and imaging of 99mTc based radiotracers with LEHR collimator on anthropomorphic phantom or realistic NCAT – SIMSET phantom followed by quantitative and qualitative images comparison.
- 5b Evolution Toolkit - Evolution Toolkit claims are supported by simulation of full count statistics using lesion simulation phantom images based on various radiotracers and collimators and by showing that SPECT image quality reconstructed with Evolution Toolkit provide equivalent clinical information but have better signal-to-noise, contrast, and lesion resolution compared to the images reconstructed with FBP / OSEM.
- 6 In clinical practice, the use of ASiR may reduce CT patient dose depending on the clinical task, patient size, anatomical location and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose to obtain diagnostic image quality for the particular clinical task.
- 7 Quantitative accuracy defined as equivalence to well counter-measured injected activity in a test phantom. Equivalence means <11% difference when comparing measured counts in SPECT studies corrected by Q.AC-reconstructed CTAC to measured counts in studies corrected by benchmark reconstructed CTAC. Measured counts are defined as average within identical ROIs positioned on SPECT reconstructed slices of homogenous 99mTc solution phantom study.
- 8 In clinical practice, the use of NM/CT 870 CZT may improve quantitation of lesions larger than 5.5 mL, depending on the clinical task, patient size, anatomical location and clinical practice. A consultation with a radiologist and a physicist should be made to determine the appropriate dose or scan time to obtain the claimed quantitation accuracy for the particular clinical task.